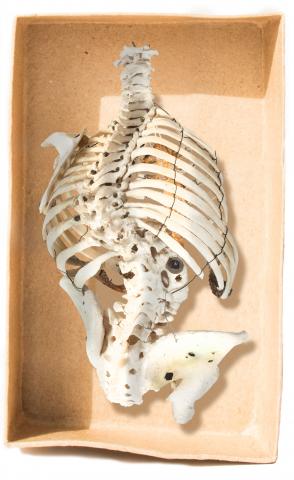
Sternum with calcified and deformed lower costal cartilages
Showing the manubrium, sternum, xiphisternum and attached costal cartilages with marked deformity of the xiphisternum and lower costal cartilages.
In the developing fetus, a ‘blueprint’ of the ribs is laid out in cartilage, which subsequently ossifies to form the rib bones. The costal cartilage is the persistent and non-ossified ventral extension of these cartilaginous models. The subsequent development of the costal cartage may be impacted by thoracic trauma, infection, ischemia, or by developmental or endocrine disorders. Calcification of the costal cartilage in adulthood is a normal process of aging.
Pathology: deformity of lower costal cartilage. Origin and pathology unknown.
Orientation: anterior

|